


The Dose Maketh the Poison: Where Are Individualized Dosing Strategies?
In the era of precision medicine, why isn't therapeutic dosing more precise? We are at worst one-size-fits-all dosing, at best trial and error adjustments.


Over 500 years ago, Paracelsus noted “Sola dosis facit venenum” – only the dose makes the poison. What he meant is that it is not the nature of the substance itself, but the amount of the substance that determines whether it is harmful.
In theory, therapeutics, whether devices or drugs, are designed to improve human physiology (efficacy) while minimizing toxicity (safety). After pre-clinical animal, or now even in silico, studies clinical trials begin. Phase I is primarily a safety assessment, but well-designed studies might test 2-4 doses of a new medicine to understand potential dose-responses. These dose responses can inform the likelihood of side effects and potential benefits. A dose response may also be suggestive that the biological pathway you are modifying with your therapeutic is more likely to play a causal role in disease.
Based on your Phase I data and occasionally paired with some statistical modeling, you choose the dose for your Phase II trial that will go head to head with placebo—the one where efficacy is truly assessed, and where much of the value is created. However, only 29% of treatments for all disease and modalities are successful at passing Phase II.

See this report from BIO. No where in this document is “dose” or “dosing” mentioned, but dosing strategy plays a major role on the success of clinical trials.
While the importance of medication dosing is well understood in theory, there is still a huge opportunity for precision. More specifically, we should use doses that are normalized to an individual’s biology or physiology— even beyond weight based dosing, we could move to functional capacity-based dosing like is done in exercise physiology.
An Example of Risk Benefit Dosing for Weight Loss
Determining the right dose which maximizes benefits and minimizes side effects is tricky.
During my time as a researcher at the NIH we sought to determine if the overactive bladder drug, mirabegron (a beta-3 agonist), could increase energy expenditure and induce weight loss via activation of brown fat (study here). Brown fat, called so due to its high amount of vascularity and mitochondrial content, can burn fat and glucose and release the energy as heat. Brown fat cells have high levels of the beta 3 adrenergic receptor, so the thought was maybe you can activate brown fat with this drug that stimulates beta 3 receptors.
50mg of B3-agonist mirabegron was FDA approved for the treatment of overactive bladder, as higher doses in early human safety studies led to increases in heart rate (likely due to off-target binding of mirabegron to beta-1 and beta-2 receptors found in the heart).
Interestingly, in our study, doses of 100mg in women could increase brown fat activity and increase energy expenditure by >10%. This means study subjects were burning off an additional ~200 calories after taking the overactive bladder drug!
However, that extra energy burned was associated with a 6.4 bpm increase in heart rate and 8.2 mmHg increase in systolic blood pressure, on average. Not ideal.
So why not find an individualized dosing strategy that maximizes benefit (calorie burning) while minimizing side effects (increased heart rate and blood pressure)? Perhaps 68mg is the right dose for one woman and 120mg is for the other. How would we go about this?
Individualized Dosing Strategies Used Today
Individualized dosing strategies used today are extremely imprecise. As a medical student rotating on the inpatient psychiatric services, I would often survey patients daily while titrating different medication doses based off clinician intuition. “Start with 20mg, see if they can “tolerate” 50mg tomorrow, and so on.” We would assess how they were feeling, were they having side effects like dry mouth, etc., depending on the medication. We also would hope their symptoms improved using this trial-and-error strategy.
In pediatrics, there was often a little more precision- weight based dosing. For example, the antibiotic amoxicillin for children over three months is dosed at 20-40mg/kg/day. At least this factors in a bit about the individual’s biology, approximating their ability to metabolize a drug.
How about a bit even more precision? Like body fat percentage-based dosing.
Another study I worked on at the NIH was to determine how much active brown fat humans have in response to drugs, or even cold rooms. We would put a person in a cold room for a few hours to activate their brown fat (its evolutionary purpose in humans and other animals is to generate heat in response to cold) and then inject them with a radioactive glucose tracer. You can track the glucose uptake in different tissues (see an example PET/CT image here demonstrating all the metabolically active brown fat).

One thing I noticed, however, was that obese patients appeared to have higher glucose uptake in their muscles, livers, and brains. This was paradoxical. Why did the subjects with impaired glucose uptake have higher glucose levels? The issue was how we individualized the units of glucose uptake. We used the mean standardized uptake value (SUVmean), which measures the amount of glucose in grams per mL of tissue.
It turns out, everybody normalized the SUVmean to total body mass when studying brown fat glucose uptake. However, white adipose tissue (fat) is significantly less metabolically active than say the muscle, liver, or brain (lean body mass). We thought to then normalize glucose uptake value to total lean body mass. Turns out, obese patients did not have more brain glucose uptake than lean people. You simply had to normalize the units to the denominator that mattered.
You can see the pronounced difference between normalized glucose uptake to total body mass (which includes metabolically inactive fat AND lean mass) versus lean body mass below.

How we diagnose and track cancer with PET/CT depends on these values! Fortunately, some PET centers normalize to lean body mass because they understand this phenomenon, but not all do. Imagine how your cancer diagnostic might be affected simply based on your body composition, that isn’t taken into consideration.
My point is that there remains an opportunity to use an individualized understanding of physiology to diagnose and treat disease.
In the era of precision medicine, why isn’t dosing more precise?
Lessons from Exercise Physiology
Individualized exercise prescription was one of the very first lessons I learned as a personal trainer and exercise physiology student back in the day. Aerobic exercise intensity could be prescribed based on an individual’s VO2max, which determines one’s maximal exercise capacity. Or more easily, you can prescribe based off of maximum predicted heart rate using the formula 220-age.
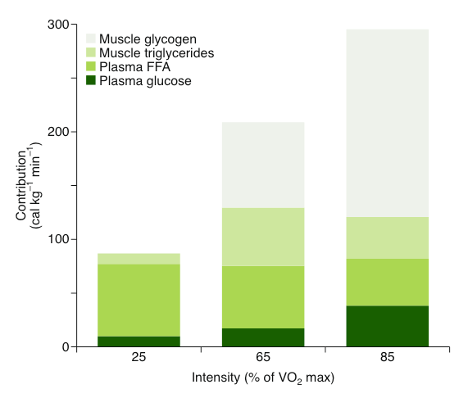
It is well understood that different physiologic and metabolic demands occur at different percentages of one’s maximal capacity. Training closer to 60% VO2max will induce greater increases in skeletal muscle vascularization and mitochondrial volume, while 85-90% of VO2max will increase the glycolytic capacity of the skeletal muscle. Walking, at close to 25% of VO2max, will cause you to burn most of your calories from fat. See this review on skeletal muscle energy metabolism and the figure below on how where your calories are burned from based on your exercise intensity.
Further, as an individual gets fitter, their VO2max will increase, and you can then adjust the exercise prescription according to how fit they are at that time.
Just as our fitness changes, the capacity of our brain changes with mood state, age, and other conditions. Wouldn’t it be nice to have dosing that could tailor interventions for brain health based on an individual’s capacity at that time?
This could be standardized in the same way that exercise physiology textbooks describe exercise prescription based on max heart rate or VO2max.
The Opportunity for Individualized Dosing
Individualized dosing for transcranial magnetic stimulation (TMS) or transcranial focused ultrasound (tFUS) seems like a major opportunity. Conduct a “maximal stimulation test” for each patient, perhaps with an EEG, or MRS, based readout.
This would happen in the research setting first in order to better characterize human physiology but could form the basis of personalized stimulation levels. Eight weeks of TMS at 80% of max stimulation may provide the right level of dosing for each patient based on their own biology, for example. Then increase the stimulation level if their max stimulation increases.
We can also learn lessons from pharmacological stress testing in cardiology. While assessing heart function with dobutamine, this drug is increased every 3 minutes from 5 to 10 mcg/kg/min in order to achieve a target heart rate. If we can use real time functional brain metrics, including EEG biomarkers taken during a stress test, rather than simply at rest, we may get closer to individualized dosing strategies. All drugs induce a sort of stress on the biological/physiological system.
A patient would enter for an EEG-based stress test, and that would determine their dosing schedule for the next several months. Progress could be adapted as usual via trial and error, but the dosing strategy would be personalized. This could be incorporated into clinical trials as the run-in period. Patients would be standardized by individualized dosing criteria, rather than a one-size-fits-all dose.
The Bigger Picture
A lot of focus in therapeutic development is spent on contemplating mechanism of action, early toxicology in animal studies. Personalized dosing is a vastly overlooked strategy to put the precision into precision medicine. Use physiologically relevant parameters to human physiology and take lessons from the stress tests in exercise physiology or cardiology.
Precision dosing is a logical approach to maximize benefit to risk ratio. We’ve known for at least half a millennia that dosing determines whether the medicine is a cure or a poison.
Oncology drugs have the narrowest of therapeutic margins yet for oral oncolytics we still use trial and error dosing. Toxicities are common at the highest doses and get better as we reduce, meanwhile the patient takes the brunt of it. Pharmacogenomics is one field I think can improve upon this yet not many places are adopting this technology. AI-based doing using your “phenome” (size, weight, kidney/liver function, family hx, germline and somatic DNA etc) is where the field needs to go. If you haven’t read Lee Hood’s work I encourage you to check it out. Hopefully,
progress is close by in this space.