



Health After the Trial
Clinical trials are a highly controlled snapshot of how new treatments can impact patient health and disease. Does this picture of health translate to benefits in the real world?

Take home concept: Clinical trials are a highly controlled snapshot of how new treatments can impact patient health and disease. Innovations in continuous health monitoring, minimally invasive wearables, and decentralized clinical trials may hold keys to ensuring that the picture of health taken at the end of a clinical trial translates to benefits in the real world. While the government is focused on ensuring public safety, and pharmaceutical companies are focused on providing financial returns to shareholders, who is incentivized to ensure human health?

Insights from Weight Loss Interventions
At the end of the 30 week intensive lifestyle change-induced weight loss competition (The Biggest Loser), contestants lost an average of >55 kgs (>120 lbs), >20% body fat, and >30% body weight loss. They had health coaches, dietary counseling, daily exercise, to an extent that many would consider extreme… but was immensely effective at treating what is now recognized as a treatable medical condition– obesity. Many of them felt healthier, and more confident, than they’d ever been at the end of the study.
Fast forward to the 2022 NEJM trial for once weekly Tirzepatide for the treatment of obesity, where the highest dose over the course of 72 weeks resulted in an average of >20% weight loss, with significant clinical benefits in fasting plasma insulin and lipids to go along with it. This is hailed as one of the biggest successes in modern medicine– the trial results eventually led to an FDA approval for chronic weight management (including priority review and fast track designation).
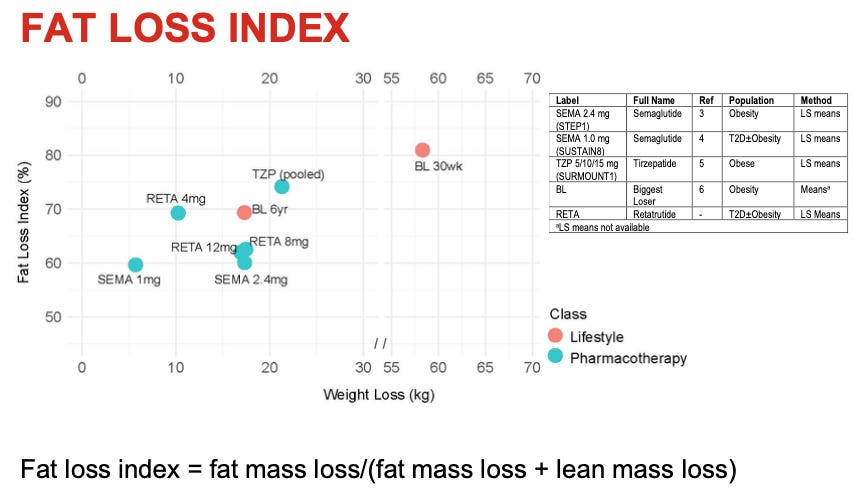
Interestingly, recently Eli Lilly plotted pharmacotherapy vs. lifestyle change for total weight lost and a fat loss index (shoutout Kevin O’Rourke for pointing me to this data). What you see is that the Biggest Loser (BL) had significantly more weight loss in 30 weeks and had the highest fat loss index (good thing, more fat lost than muscle). What you also see is “BL 6yr,” which refers to the study conducted at the NIH by Kevin Hall’s lab that examined body composition and energy expenditure in the Biggest Loser contestants 6 years after the end of the show.
Fun fact, I measured the Resting Energy Expenditure on all of these contestants. It was ~5:30am on a Saturday & Sunday on a cold day in Bethesda, MD– I biked from my house in DC along the Capital Crescent Trail because the metro wasn’t open early enough for me to get there on time.
What is fascinating is that although these contestants gained back an average of 40 kgs (~90 lbs) over the course of 6 years, they still were in a better place than nearly all weight loss drugs and equivalent to Tirzepetide for weight loss and fat loss. We also know that in the real world, patients also gain back most of the weight they’d lost while on the drugs, mitigating much of the success of a drug intervention.
Now, while these contestants are arguably in a healthier place than they were before any intervention, imagine if they could hold on to a larger fraction of the weight loss, and more importantly, health benefits. Extend this to the patients on weight loss drugs. Now extend this to any FDA approved treatment.
How can we get better at ensuring “health after the trial”?
There’s a Government Approach, beginning with the 21st Century Cures Act
“The 21st Century Cures Act (Cures Act), signed into law on December 13, 2016, is designed to accelerate medical product development and bring new innovations and advances faster and more efficiently to the patients who need them… the [FDA] has created a framework for evaluating the potential use of real-world evidence (RWE) to help support the approval of a new indication for a drug already approved… or to help support or satisfy drug postapproval study requirements” - Framework for FDA’s Real World Evidence Program
The FDA may obtain real world data derived from electronic health records, medical claims and billing data, patient generated data, and data gathered from other sources such as mobile devices. Much of their efforts have focused on safety. The FDA is tasked with ensuring that products they review that are released to the public do as little harm as possible. They often rely on the report of adverse events so that they can eventually recall drugs, or put something like a Black Box warning on certain medications.
The FDA states: “However, the use of [Real World Evidence] to support effectiveness determinations is much more limited.”
“On Sept. 14, 1988, FDA created in CDER the Therapeutic Inequivalence Action Coordinating Committee (TIACC) to identify and evaluate reports of therapeutic failures and toxicity that could indicate that one product is not equivalent to another similar product.” This committee was put into place to see if generic drugs worked as well as brand name drugs. If I were a betting man, I’d guess this lack of efficacy is due to real world drug usage (ie. not in a highly controlled trial setting) rather than a difference in drug formulation (see previous citation). Again, this is to mitigate harm, not to ensure health.
Stakeholder Incentives in Patient Health Outcomes: A Systems Perspective
Let's examine who is (theoretically) incentivized to ensure real-world health outcomes align with therapeutic prescription. While the FDA oversees safety, the effectiveness landscape is more complex:
Government: Strong Direct Incentives ✓ The public health mandate coupled with substantial healthcare spending (e.g. in 2021, Medicare Part D spent $216 billion on prescription drugs, not even accounting rebates paid to pharmacy benefit managers) creates powerful incentives for ensuring treatment effectiveness. If you were spending that much on treatments, wouldn’t you want 1) to pay only as long as needed, and 2) ensure they are both safe AND effective? Perhaps this would be an evolution of FDA responsibility.
Clinical Practitioners: Mixed Implementation Capacity ⚖️ While clinicians are fundamentally motivated by patient health outcomes, systemic constraints affect their ability to optimize treatment effectiveness. The shift toward evidence-based guidelines, while important for standardization, can create a lag between emerging real-world evidence and clinical practice adaptation.
Insurance: Not Yet The traditional insurance model, operating on short-term payment cycles, fundamentally misaligns with patient health trajectories that span decades. Even sophisticated actuarial modeling cannot fully bridge this gap when patients frequently switch insurers, diluting accountability for long-term health outcomes. However, value-based care models are emerging as a transformative solution. By directly linking payment to health outcomes rather than service volume, these models create powerful incentives for insurers to invest in preventive care and long-term health management.
Pharmaceutical Industry: Indirect Health Alignment 〰️ The current revenue model based on recurring sales creates a potential misalignment with curative outcomes. However, this represents a structural economic challenge rather than intent. If fewer patients have the diagnosis due to efficacy of therapy (rather than life long support), the drug will be sold less. The solution likely lies in upstream development incentives and innovative business models that reward health outcomes. (e.g. are key health metrics tracked on patients after the trial)
Innovation Ecosystem: Emerging Solutions ↗️ Key opportunities include:
Advanced compliance monitoring systems integrated with post-marketing surveillance studies
Passive health metric collection through sophisticated wearables
Development of functional health endpoints that bridge biological markers with meaningful health outcomes
Current Innovations in Health-Oriented Trial Design for Brain Diseases
Emerald Innovations (MIT spinout), a touchless sensor and machine learning platform for health analytics, offers a unique solution. By using minimally invasive monitoring alongside clinical trials, they enable sensitive biomarkers and a solution for decentralized trials. They are partnering with Verge Genomics in order to obtain objective metrics in patients with ALS. The exciting thing is that true objective functional measures might be integrated as endpoints for the FDA, aligning trial success with patient outcomes.
Another intriguing partnership is between Aspen Neuroscience, Emerald Innovations, and Rune Labs in order to obtain digital biomarkers for a Parkinson’s trial. Emerald is providing the contactless biosensors (sensing movement via radiowaves) and Rune Labs is providing the clinical development platform to “objective, long-term (pre-treatment) motor and sleep symptom capture, to provide data on each patient’s rate of disease progression.”
Obtaining measures of health and function before, during, and after treatment is necessary to fit within the current biomedical and current clinical trial framework. With longitudinal measures we will better be able to engage with patients without the need for intensive trial approaches, and ideally be able to ensure health after the trial. In other words, capturing health data in the context of pre, during, and post intervention is likely to generate the level of quality needed.
The Future of Real World Data and the Convergence of Biotech & Pharma with Consumer Health
Future efforts will build on the increasing demand for innovative, real world trial design, via decentralized clinical trials (see ARPA-H’s Advancing Clinical Trial Readiness (ACTR) initiative) and the FDA’s Real World Evidence Guidance. We will likely see traditional biotech and pharma companies take advantage of these routes.
Another trend is the convergence of consumer tech gaining clinical trial grade credibility… Whoop continues to publish peer reviewed data (e.g. a biomarker for pre-term birth, and cardiovascular parameters across the menstrual cycle), and Oura launching its first clinical trial for reducing arterial stiffness, we will increasingly see the role of everyday wearable companies solving this problem. A major challenge remains for improving brain health via wearables, and I’m excited to see companies pop up to improve brain health in the real world.
I’m excited for a world that moves towards health, function, and quality of life as end goals of biomedical innovation.